 |
||
 Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases
Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases
|
||
|
|
|
|||||||
| Abstracts and Articles Discuss Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases in the Main forums forums; Int J Med Sci 2010; 7:155-159 ©Ivyspring International Publisher Research Paper Percutaneous laser disc decompression for thoracic disc ... |
 |
|
|
LinkBack | Thread Tools | Display Modes |
 03-18-2011, 01:20 PM
03-18-2011, 01:20 PM
|
||||
|
||||
|
Int J Med Sci 2010; 7:155-159 ©Ivyspring International Publisher
Research Paper Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases Scott M.W. Haufe1,3 , Anthony R. Mork2,3, Morgan Pyne4, Ryan A. Baker4 1. Chief of Pain Medicine and Anesthesiology 2. Chief of Spine Surgery 3. MicroSpine, DeFuniak Springs, FL 32435, USA 4. University of South Florida Medical Student How to cite this article: Haufe SMW, Mork AR, Pyne M, Baker RA. Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases. Int J Med Sci 2010; 7:155-159. Available from Percutaneous laser disc decompression for thoracic disc disease: report of 10 cases Abstract Background: Discogenic pain or herniation causing neural impingement of the thoracic vertebrae is less common than that in the cervical or lumbar regions. Treatment of thoracic discogenic pain usually involves conservative measures. If this fails, conventional fusion or discectomy can be considered, but these procedures carry significant risk. Objectives: To assess the efficacy and safety of percutaneous laser disc decompression (PLDD) for the treatment of thoracic disc disease. Methods: Ten patients with thoracic discogenic pain who were unresponsive to conservative intervention underwent the PLDD procedure. Thoracic pain was assessed using the Visual Analog Scale (VAS) scores preoperatively and at 6-month intervals with a minimum of 18-months follow-up. Patients were diagnosed and chosen for enrollment based on abnormal MRI findings and positive provocative discograms. Patients with gross herniations were not included. Results: Length of follow-up ranged from 18 to 31 months (mean: 24.2 mo). Median pretreatment thoracic VAS score was 8.5 (range: 5-10) and median VAS score at final follow-up was 3.8 (range: 0-9). Postoperative improvement was significant with a 99% confidence interval. Of interest, patients generally fell into two groups, those with significant pain reduction and those with little to no improvement. Although complications such as pneumothorax, discitis, or nerve damage were possible, no adverse events occurred during the procedures. Limitations: The study is limited by its small size and lack of a sham group. Larger controlled studies are warranted. Conclusions: With further clinical evidence, PLDD could be considered a viable option with a low risk of complication for the treatment of thoracic discogenic pain that does not resolve with conservative treatment. Keywords: back pain, minimally invasive surgery, laser, intervertebral disc, spine surgery Conflict of Interest The authors have declared that no conflict of interest exists. Author contact Corresponding author: Scott M.W. Haufe, M.D., 101 MicroSpine Way, DeFuniak Springs, FL 32435. Phone: 888-642-7677; Fax: 850-892-4212; Email: Haufe@MicroSpine
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org 
|
|
03-18-2011, 01:30 PM
|
||||
|
||||
|
Background and objectives
Percutaneous laser disc decompression (PLDD) is a minimally invasive treatment option for vertebral disc herniation refractory to conservative treatment. PLDD was first used in 1986 and received approval from the U.S. Food and Drug Administration in 1991 (1). Based on the reduced risk associated with less invasive procedures, PLDD has increased in popularity, with reportedly over 30,000 PLDD procedures performed in 2001 (2). PLDD is performed under local anesthesia via a laser fiber percutaneously inserted into the nucleus pulposus. Laser energy is applied through the fiber, resulting in vaporization of nucleus pulposus contents (3). Improvement in discogenic pain with PLDD is based upon laser-induced evaporation of water within the disc; this results in a very slight decrease in disc size due to water loss. Because the intervertebral disc is essentially a closed hydraulic system, a small decrease in volume leads to a significantly larger decrease of intradiscal pressure; in vitro experiments confirm this (4,5). The short term decrease in pressure is due to evaporation of water content within the nucleus pulposus; long term effects are thought to be due to protein denaturation, which limits the ability of the nucleus to resorb additional water and reduces stiffness of the disc (3,6,7). This hypothetically results in a more even distribution of weight across the intervertebral disc (8). Consistent with a lumbar location for the majority of intervertebral disc herniations, most published studies have focused on the use of PLDD for the treatment of lumbar disc disease. Thoracic discogenic pain or herniation causing neural impingement is less common than that in the cervical or lumbar regions. Certain impact injuries, such as parachute landings, can result in thoracic disc damage. Invasive treatment of such injuries often involves a thoracotomy procedure with either a discectomy or fusion implantation. Although many studies have been done on lumbar and cervical PLDD procedures, few have been done on the thoracic region. In order to assess the efficacy and safety of PLDD for the treatment of thoracic disc disease, we performed a study of ten patients with thoracic discogenic pain who were unresponsive to conservative intervention. Methods We performed a prospective study of ten patients (8 male and 2 female) with an age range of 35-73 years. All patients presented with mid-thoracic axial (n=7) or radicular (n=1) pain that failed to improve with conservative management, which included typical modalities such as physical therapy, pain medication, and epidural steroid injections. Physical examination revealed localized thoracic pain without recreation of symptoms with palpation. The pain was either centralized or radiating to one side. There was no facet tenderness present. All the patients had negative facet injections, to evaluate for the possibility of facet joint pain as the underlying cause. The patients had positive discograms that correlated to their pain; in the case of the individual with radicular symptoms, she had total relief of her pain with a thoracic nerve root block, confirming this as the source of her pain. All patients were diagnosed with thoracic discogenic pain based on MRI and provocative discogram results. Magnetic resonance imaging (MRI) findings that were considered abnormal included changes described as irregular nuclear shape, reduced disc height, hypo-intense disc signal, annular tears, high intensity zones, endplate changes, and Modic changes (9,10,11). All patients underwent diagnostic injections to confirm the source of their pain; these injections included either thoracic nerve root blocks for radicular symptoms and/or provocative discograms (12). The provocative discograms involved low-pressure injections of at least three disc levels and one of the levels was utilized as a control. Thoracic discography has been utilized as a controversial confirmatory test for discogenic pain for some time with debatable results (13,14). Studies show false positive results with discograms to be as high as 25% (13,15). A recent systematic review reported the published evidence to be of low quality (16). The authors identified only two studies by the same authors for inclusion, each over 10 years old. They recommended that other methods may be equally effective. Due to the lack of established accuracy of discography, we required the combination of an abnormal MRI and a positive provocative discogram to diagnose intervertebral discs as the source of pain and to identify potential study participants. It was felt that gross herniations producing significant cord compression would be better treated with a laminotomy approach, and that not enough disc material would be removed to resolve the stenosis in such situations. Thus only patients with contained disc protrusions were considered for PLDD and patients with gross herniation were removed from the study and sent for laminotomy or conventional discectomy. Patients' chosen for the procedure reported their thoracic pain using the Visual Analog Scale (VAS) pain scores at baseline. Posttreatment, patients were evaluated every six months via telephone call or direct patient contact for at least 18 months. The patient was specifically asked to address the pain level of the thoracic spine region and not the body as a whole. This was done to eliminate patients with short-term improvement from introducing bias. A double-blinded study would have been preferable with a sham group but was not possible at our facility. The procedure begins with a properly prepped and draped patient in the prone position. All patients received intravenous (IV) antibiotics prior to the procedure. Cefofloxin was utilized unless there was an allergy, in which case ciprofloxin was used. Mild sedation was used during the procedure and the patient was able to converse with the surgeon in order to express any unusual pain. Sedation involved a combination of benzodiazepines and opiates. Fluoroscopy was utilized during the procedure for proper count of the thoracic vertebrae and to determine the entry site. The entry site was similar in position to a typical thoracic discogram and was approximately 3 inches lateral to the midline of the spine. Caution was necessary due to the lung fields being close to the needle entry site, increasing the risk of pneumothorax. Once the entry site was determined, the skin and deeper tissues were anesthetized with a mixture of 0.25% bupivacaine and 1% lidocaine with epinephrine via a 27-gauge needle. A 15 blade was used to create a stab incision of approximately ¼ inch. Through the incision, an 18-gauge, 3.5-inch spinal needle was inserted and the needle was guided into the middle of the disc using fluoroscopy. Positioning was confirmed via anterior and lateral x-ray views. Once properly placed, a direct firing holmium laser (diameter 0.5 mm) at 20 watts and 10 repetitions per second (6030-10405 Joules, mean 7633) was utilized in short bursts to vaporize the inside of the disc. In most cases these burst were of ten second intervals; the patient usually complained of burning mid back pain which limited the time per lasing period. After the lasing periods, the disc was cooled with normal saline (at least 100 ml) mixed with cefazolin (unless there was an allergy). Saline irrigation was performed after, not simultaneously with, laser application due to the size of the diameter of the working environment and because a running irrigant would reduce the laser's effectiveness and thus increase operating times. Total lasing time was approximately 3 minutes, but varied from 80 seconds to 300 seconds. In most cases, the end point was when the pressure in the disc was reduced and injection of the normal saline occurred without any resistance. At this point the needle was removed and either the next disc was commenced or the procedure was finished. Closure involved a single steri-strip over the incision. No sutures were used. Tegraderm and 2x2 gauze was placed over the wound. Results All ten patients tolerated the procedure well. There were no complications. Expected possible complications included those seen with thoracic discogram and laser usage such as infection or discitis, pneumothorax, nerve injury, and burn injuries (14). Each patient had a post procedural chest x-ray to rule out pneumothorax; no pneumothorax was seen. Length of follow-up ranged from 18 to 31 months (mean: 24.2 months). Patients were asked to assess their thoracic pain via a VAS score preoperatively and at final follow-up visit. Median VAS score pretreatment was 8.5 (range: 5-10) and median VAS at final follow-up was 3.8 (range: 0-9). Six of ten patients' scores improved by at least 6 points; one patient improved by 1 point and three patients' scores did not improve. No patients reported worsening of symptoms. Results are summarized in Table 1. No side effects were reported, and no adverse events occurred during the procedure. 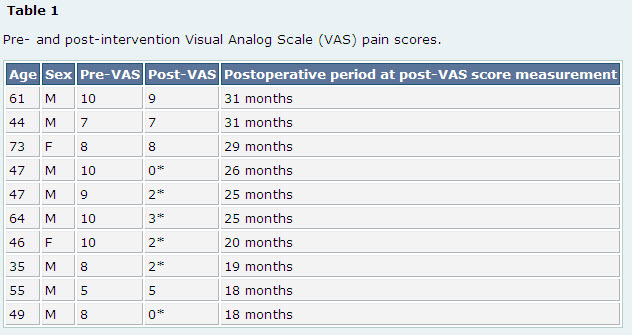 M: Male F: Female Pre-VAS: Visual Analog Scale pain score prior to PLDD. Post-VAS: Visual Analog Scale pain score after PLDD. *Patients (n=6, 60%) experiencing at least 6 point improvement in VAS postoperatively. Note that remaining patients reported minimal or no improvement. Discussion Thoracic disc disease is much less common than that of lumbar and cervical discs. However, certain types of impact, such as parachute landing, carry an increased risk of thoracic disc injury. Optimal treatment of thoracic discogenic pain is identical to that of disease of other spinal regions, i.e. aggressive medical management with anti-inflammatory medication, hot compresses, and physical therapy. Although epidural steroid injections are questionably proven to help with such cases, they are commonly utilized and are thus considered as a conservative therapy. Patients who fail to improve with conservative treatments have several invasive options, including conventional thoracotomy procedures for discectomy and fusion, posterior fusion, laminotomy, and disc decompression. These procedures generally carry significant risk and down time for potential patients. Several different types of lasers are used when performing PLDD. High energy laser carriers the risk of tissue burns, but low energy lasers may be insufficient to adequately induce vaporization (1). Lasers near the infrared region currently used in PLDD include neodymium:ytrium-aluminum garnet laser [Nd:YAG], holmium:ytrium- aluminum-garnet laser [Ho:YAG], and diode laser. Lasers with visible green radiation include double-frequency Nd:YAG laser and potassium-titanyl-phosphate [KTP] laser. Most lasers use a 3mm outer cannula combined with a fiberoptic viewing cable (17). There is no clear consensus regarding the most effective and safe laser or the ideal wavelength that should be used (1). Most lasers provide 1200 Joules of energy in a pulsatile fashion (17). PLDD is a minimally invasive technique that reduces intradiscal pressure by vaporization of a small volume of water within the nucleus pulposus. This results in decreased overall pressure and a more even distribution of weight across the disc, with subsequent relief of discogenic pain. PLDD is performed most commonly for lumbar disc disease, and published reports on the efficacy of PLDD in thoracic discogenic pain are lacking. The majority of PLDD studies are of small size and observational in nature; thus the true efficacy of this technique is uncertain (18). Multiple case series have reported success with PLDD for the treatment of lumbar discogenic pain (15,19-30); however, no randomized controlled trials have been performed. A systematic review by Singh et al. reported that conclusive evidence of efficacy is lacking, and large scale, comparative trials are warranted given the potential benefit of PLDD (18). The majority of authors report fair to good improvement in approximately 75% of patients, most commonly based upon the McNab scale. Immediate relief is reported to occur in 75-90% of patients. Rates of complication are low, the most common being septic or aseptic discitis, disc rupture, epidural hematoma, and nerve root damage (24,30-32). A recent study on thoracic PLDD procedures by Hellinger et al. reported improvement in 41 of 42 patients six weeks after percutaneous laser decompression and nucleotomy (PLDN) (35). The authors reported three adverse events: one occurrence each of pneumothorax, pleurisy, and spondylodiscitis. Long-term outcome was not reported and thus it is unknown if their results extended beyond the study period of 6 weeks. In our study, six of ten patients reported significant pain relief based on Visual Analog Scale pain scores concerning their thoracic pain issue. Utilizing a paired student's t-test, the differences between the pre- and post-treatment groups showed greater than a 99% confidence interval confirming that the improvement was indeed significant. The 60% improvement level noted is slightly lower, although still in agreement, with published reports of PLDD in patients with lumbar disc disease (15,19,34). Of interest, patients appeared to fall into two main groups: those gaining significant improvement and those receiving little or no improvement at all. In reviewing the patients who failed treatment, we could not distinguish any specific features, such as MRI findings or other clinical data, which could be utilized to screen these potential failed patients in the future. Importantly, no adverse events occurred in the intra- or postoperative period. Intervention for the treatment of thoracic disc disease carries a risk of pneumothorax, and particular concern was given to this possibility during the intervention. No patient developed pneumothorax, and no evidence of discitis, infection, or nerve injury was noted. Conclusion This is one of the first reports of the successful application of PLDD for the treatment of thoracic discogenic pain. Although the study group is small with only ten patients, six out of the ten patients reported significant improvement at long-term (greater than 18 month) follow-up, and no adverse events were reported. PLDD could be considered a viable option with a low risk of complication for the treatment of thoracic discogenic pain that does not resolve with conservative treatment. Nonetheless, due to the small study size, we recommend a larger double-blinded study to confirm our results.
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org Last edited by mmglobal; 03-18-2011 at 01:43 PM.
|
|
03-18-2011, 01:31 PM
|
||||
|
||||
|
References
1. Goupille P, Mulleman D, Mammou S, Griffoul I, Valat JP. Percutaneous laser disc decompression for the treatment of lumbar disc herniation: a review. Semin Arthritis Rheum. 2007;37:20-30 2. Choy DS, Case RB, Fielding W, Hughes J, Liebler W, Ascher P. Percutaneous laser nucleolysis of lumbar disks. N Engl J Med. 1987;317:771-772 3. Schenk B, Brouwer PA, van Buchem MA. Experimental basis of percutaneous laser disc decompression (PLDD): a review of literature. Lasers Med Sci. 2006;21:245-249 4. Choy DS, Michelsen J, Getrajdman G, Diwan S. Percutaneous laser disc decompression: an update--Spring 1992. J Clin Laser Med Surg. 1992;10:177-184 5. Choy DS, Altman P. Fall of intradiscal pressure with laser ablation. J Clin Laser Med Surg. 1995;13:149-151 6. Choi JY, Tanenbaum BS, Milner TE. et al. Theramal, mechanical, optical, and morphologic changes in bovine nucleus pulposus induced by Nd:YAG (lambda = 1.32 microm) laser irradiation. Lasers Surg Med. 2001;28:248-254 7. Castro WH, Halm H, Jerosch J, Schilgen M, Winkelmann W. [Changes in the lumbar intervertebral disk following use of the Holmium-Yag laser--a biomechanical study]. Z Orthop Ihre Grenzgeb. 1993;131:610-614 8. Kutschera HP, Lack W, Buchelt M, Beer R. Comparative study of surface displacement in discs following chemonucleolysis and lasernucleotomy. Lasers Surg Med. 1998;22:275-280 9. Peng B, Hou S, Wu W, Zhang C, Yang Y. The pathogenesis and clinical significance of a high-intensity zone (HIZ) of lumbar Intervertebral disc on MR imaging in the patient with discogenic low back pain. Eur Spine J. 2006May;15(5):583-7 10. Finch P. Technology Insight: imaging of low back pain. Nat Clin Pract Rheumatol. 2006;2(10):554-61 11. Kjaer P, Leboeuf-Yde C, Korsholm L, Sorensen JS, Bendix T. Magnetic resonance imaging and low back pain in adults: a diagnostic imaging study of 40 year-old men and women. Spine. 2005;30(10):1173-80 12. Choy DS. Percutaneous laser disc decompression (PLDD): twelve years' experience with 752 procedures in 518 patients. J Clin Laser Med Surg. 1998;16:325-331 13. Singh V. Thoracic discography. Pain Physician. 2004;7(4):451-8 14. Carragee EJ, Alamin TF, Carragee JM. Low-pressure positive discography in subjects asymptomatic of significant low back pain illness. Spine. 2006;31(5):505-9 15. Guyer RD, Ohnmeiss DD. Lumbar discography. Spine J. 2003;3(3 Suppl):11S-27S 16. Singh V, Manchikanti L, Shah RV. et al. Systematic review of thoracic discography as a diagnostic test for chronic spinal pain. Pain Physician. 2008;11:631-42 17. Singh V, Derby R. Percutaneous lumbar disc decompression. Pain Physician. 2006;9:139-46 18. Singh V, Manchikanti L, Benyamin RM. et al. Percutaneous lumbar laser disc decompression: a systematic review of current evidence. Pain Physician. 2009;12:573-88 19. Choy DS, Ascher PW, Ranu HS. et al. Percutaneous laser disc decompression. A new therapeutic modality. Spine. 1992;17:949-956 20. Sherk HH, Rhodes A, Black J, Prodoehl JA. Results of percutaneous lumber discectomy with lasers. State of the Art Reviews Laser Discectomy. Philadelphia: Hanley & Belfus. 1993:141-150 21. Choy DS. Techniques of percutaneous laser disc decompression with the Nd:YAG laser. J Clin Laser Med Surg. 1995;13:187-193 22. Casper GD, Mullins LL, Hartman VL. Laser-assisted disc decompression: a clinical trial of the holmium:YAG laser with side-firing fiber. J Clin Laser Med Surg. 1995;13:27-32 23. Casper GD, Hartman VL, Mullins LL. Results of a clinical trial of the holmium:YAG laser in disc decompression utilizing a side-firing fiber: a two-year follow-up. Lasers Surg Med. 1996;19:90-96 24. Choy DS. Clinical experience and results with 389 PLDD procedures with the Nd:YAG laser, 1986 to 1995. J Clin Laser Med Surg. 1995;13:209-213 25. Chambers RA, Botsford JA, Fanelli E. The PLDD registry. J Clin Laser Med Surg. 1995;13:215-219 26. Bosacco SJ, Bosacco DN, Berman AT, Cordover A, Levenberg RJ, Stellabotte J. Functional results of percutaneous laser discectomy. Am J Orthop. 1996;25:825-828 27. Siebert WE, Berendsen BT, Tollgaard J. [Percutaneous laser disk decompression. Experience since 1989]. Orthopade. 1996;25:42-48 28. Nerubay J, Caspi I, Levinkopf M. Percutaneous carbon dioxide laser nucleolysis with 2- to 5-year followup. Clin Orthop Relat Res. 1997:45-48 29. Gevargez A, Groenemeyer DW, Czerwinski F. CT-guided percutaneous laser disc decompression with Ceralas D, a diode laser with 980-nm wavelength and 200-microm fiber optics. Eur Radiol. 2000;10:1239-1241 30. Knight M, Goswami A. Lumbar percutaneous KTP532 wavelength laser disc decompression and disc ablation in the management of discogenic pain. J Clin Laser Med Surg. 2002;20:9-13 31. Tassi GP. Preliminary Italian experience of lumbar spine percutaneous laser disc decompression according to Choy's method. Photomed Laser Surg. 2004;22:439-441 32. Black W, Fejos AS, Choy DS. Percutaneous laser disc decompression in the treatment of discogenic back pain. Photomed Laser Surg. 2004;22:431-433 33. McMillan MR, Patterson PA, Parker V. Percutaneous laser disc decompression for the treatment of discogenic lumbar pain and sciatica: a preliminary report with 3-month follow-up in a general pain clinic population. Photomed Laser Surg. 2004;22:434-438 34. Grönemeyer DH, Buschkamp H, Braun M, Schirp S, Weinsheimer PA, Gevargez A. Image-guided percutaneous laser disk decompression for herniated lumbar disks: a 4-year follow-up in 200 patients. J Clin Laser Med Surg. 2003;21:131-138 35. Hellinger J, Stern S, Hellinger S. Nonendoscopic Nd-YAG 1064 nm PLDN in the treatment of thoracic discogenic pain syndromes. J Clin Laser Med Surg. 2003;21:61-66
__________________
1997 MVA 2000 L4-5 Microdiscectomy/laminotomy 2001 L5-S1 Micro-d/lami 2002 L4-S1 Charite' ADR - SUCCESS! 2009 C3-C4, C5-C6-C7, T1-T2 ProDisc-C Nova Summer 2009, more bad thoracic discs! Life After Surgery Website President: Global Patient Network, Inc. Founder: www.iSpine.org
|
|
03-18-2011, 03:11 PM
|
|||
|
|||
|
thanks for posting that Mark, it is very interesting reading and something i would consider if my other thoracic discs act up (they better not)
judy
__________________
2007 ACDF 4-7 2008 hip , knee scope, hip replacement 2009 thoracic T-5 thru T-11fusion 2009 VATS T7-8, posterior only T11-12. removal of thoracic hard wear 2010 lung surgery 2010 T2-L2 kyphosis correction 2010 Kyphoplasty T-3, T-4 2011 Cervical osteotomy ,revision C4-T5 2011 Foot surgery 2011 Revision fusion T7 thru L4/laminectomy 2012 Hammertoe correction left foot 2012 Revision fusion T-12 thru L5 2012 Revision fusion L4-L5
|
|
03-19-2011, 10:22 AM
|
||||
|
||||
|
What can I say. After studying so much about PLDD I can only say THANK YOU DR. CHOY for bringing this wonderful technique to us.
In Croatia, we use PLDD very often. Mainly for contained herniations (bulges, protrusions). Sometimes we use bipolar technique (in same time booth sides -left and right) to shrink annular tears. Dr. Saftic's results with this technique is excellent, around 80% of patients are happy.
__________________
"The world of spinal medicine, unfortunately, is producing patients with failed back surgery syndrome at an alarming rate" 2005 - 2012: Rich personal experience with spinal disorders and various treatments (surgical, therapeutic, diagnostic) Co-Founder: Vertebris Internationl Spine Hospital Founder: Spinoteka - Society for Spine Diseases
|
|
| Bookmarks |
| Tags |
| back surgery, decompression, disc, laser, percutaneous, pldd, spine surgery, thoracic |
|
|






 Linear Mode
Linear Mode



