(continued from previous post)
If you think that this is a Charite’ issue, you are mistaken. While the failure mode of the Charite’ seems to be worse, you avoid the failure mode by getting the surgery done properly. Poorly located or poorly sized discs are a problem no matter which disc you use. I see similar problems with other designs. You can’t put any of them in improperly and not have disasters. I will say again and again… there is a difference between the unavoidable failure that all spine surgeons experience and a failure that absolutely would not have happened if the surgery was done properly.
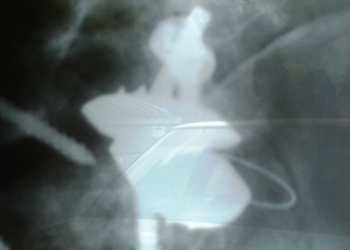
Here is another case that is similar. Look at the pre-migration picture for the placement of the plates. The prosthesis is right-side-up, but it’s so anteriorly located that the cleats are literally riding on the anterior ridge. Unfortunately, the post-migration xray is oblique and of poor quality, but you can see the lower plate has migrated out and rotated 90 degrees as it migrated out and like John, the core was expulsed. Do you think it is a coincidence that the plate that was hanging off the front of the body is the one that expulse.

Any experienced ADR surgeon should look at the interoperative images and see that while this MIGHT stay put, this is just as likely, a disaster waiting to happen. In every ADR surgery I’ve observed (with the exception of one), there are literally dozens of xrays taken to insure proper positioning. None of the surgeons I’ve seen doing ADR (with the exception of one), would look at an image like this and consider the job of placing the prosthesis to be done – time to close. (I’ve seen close to 200 arthroplasty procedures in more than a dozen centers, more than a dozen implants.)
This patient was told that the reason for the expulsion was because of the fusion below. I have MANY clients with similar configurations. That placement is problematic without regard to the adjacent disc. ADR adjacent to fusion is not problematic when properly placed, properly sized, etc.
I really appreciate that kc0iet and Havanna have come forward and started this discussion. This is NOT about the design of the Charite’. This is NOT about the general risk of ADR surgery. The two cases that I have written about in this post are 100% carelessness, poor implantation that should NEVER HAVE HAPPENED. Both of these patients had every reason to look for success or at least a chance of success because they were going to a surgeon with a great deal of ADR experience. Sadly, what they got was something completely different.
Please note that the patient with the fusion was done on the same day as the MrBee disaster in August 2004. That is also the same day as the Carmont disaster. One would think that they would have learned that such anterior placement is a bad idea. We have to ask, why are they still making the same avoidable mistakes in October 2005? The surgeon gets to choose when the prosthesis is appropriately placed. They look and say, "yeah, that's good", or "no, it needs to go further back." With the Charite' they have the option taking it out and starting again. (I've seen that done many times.) It is a choice they make to close the patient when they feel that it's appropriately placed. These cases are NOT, "all surgeons have problems!"
I'm sorry this is so strong. I get very agitated when I have to discuss Stenum because I've seen so many of these unnecessary, avoidable disasters that result in lives ruined. I apologize to all the happy Stenum patients who had a wonderful experience and love them. I know a lot of happy Stenum patients. Some of them are happy campers in spite of poor implantations. Some have success with good work done. But, what I've seen as the steady stream of avoidable disasters is unforgivable. As my friend said, if you are an airline pilot or a surgeon, you have to keep learning and improving. Sadly, for the complacency shown in these cases and so many others, the patients paid such a severe price.
All the best,
Mark